12 important questions your child needs you to ask

1. Is the Vaccine safe?
Mounting evidence in countries administering the vaccine to children shows a significant number of serious side effects in young people.
The UK’s Joint Committee on Vaccination and Immunisation produced a report on 3rd September 2021 that assessed that the potential risks to healthy children from the covid vaccine outweighed the benefits.
Analysis of US data reveals that Covid vaccines like Pfizer are the most dangerous vaccines in human history. They are 800 times more deadly than the smallpox vaccine, which was the previous record holder. One author has estimated that Covid vaccines could kill as many as 117 children for every death they prevent.
Serious adverse effects and vaccine-related deaths are reported around the world via government monitoring schemes - in the UK via the Yellow Card system [1], in the US via the Vaccine Adverse Event Reporting System (VAERS) [2], in Europe via Eudravigilance [3] and in New Zealand via “CARM”, the Centre for Adverse Reactions Monitoring (reports available through Medsafe).
In the US, 160 children under the age of 18 (as of 14 January 2022) have been reported to have died following Covid-19 vaccination. Through to 14 January 2022, reports to VAERS for all ages included 22,193 Covid vaccine related deaths, 118,684 hospitalisations, 11,260 heart attacks and 27,674 cases of myocarditis/pericarditis.
In Europe to 15 January 2022, the EU pharmacovigilance database reported 1,624,526 adverse reactions for the Pfizer vaccine and 17,054 fatalities.
Official data from the Office of National Statistics shows deaths among female children in the UK increased by 57% against the five-year average since the Covid-19 vaccine was introduced to children over 12 years. [4]
Recently, New Zealand’s Medsafe added Adverse Event Following Immunisation (AEFI) for children, to their table titled ‘Summary of investigations into possible safety signals’. As of 31 December 2021, a total of 4,173 AEFI reports in children aged 10-19 have been filed, along with reports of 7 deaths in the age group 10-29 years.
And we can be fairly certain that adverse events are under-reported rather than over-reported. A 2010 Harvard study found that fewer than 1% of all vaccine-related injuries are reported to VAERS in the US. [5] The UK Government estimates that the Yellow Card system captures fewer than 10% of adverse drug reactions.[6]
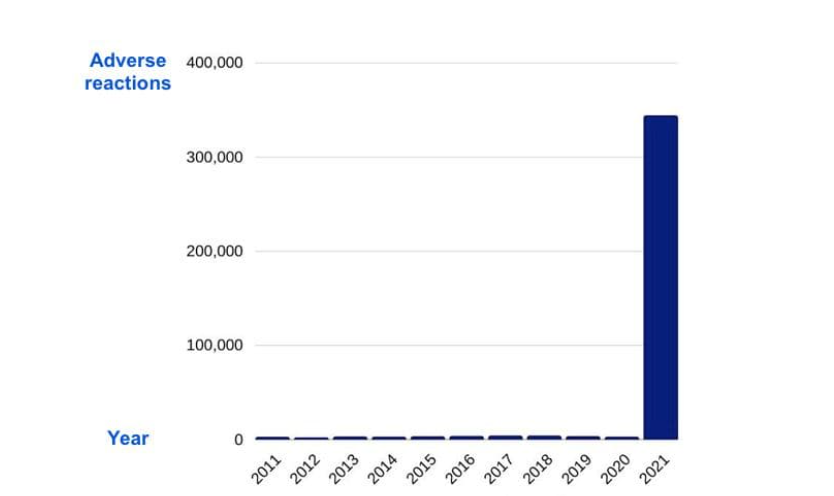
As noted above, adverse reactions to the vaccines are being reported to government monitoring schemes at a much higher rate than is usual with vaccines (see graph below).
MHRA Adverse Drug Reaction (ADR) reports for all vaccines in the last 10 years (as at Aug 2021)
Some adverse events are more common in the young. For example, doctors are seeing increasing reports of myocarditis (inflammation of the heart muscle) after vaccination, particularly in young males aged 12-17. Myocarditis has been reported at 13.6 times the expected rate in 16 to 19 year old males after their second Pfizer vaccine (10.1056/NEJMoa2109730). The risk of myocarditis in 12-15 year old boys after vaccination has been found to be 3.7 to 6.1 times higher than the risk of hospitalisation from Covid, even under conditions of moderate to high Covid-19 incidence (https://www.medrxiv.org/content/10.1101/2021.08.30.21262866v1.full.pdf).
Pfizer said the clinical development programme was “too small to detect any potential risks of myocarditis associated with vaccination” and that “myocarditis/pericarditis in participants 5-12 years of age will not be studied until AFTER the vaccine is authorised for children.”

2. What are the chances of my child getting seriously ill or dying from Covid?
Children and young people have a near-zero risk of getting seriously ill or dying from Covid. Most children who catch Covid will have no symptoms, or only very mild symptoms. [1]
The survival rate of children and young people with a positive Covid test in England was found to be 99.995% (https://pubmed.ncbi.nlm.nih.gov/34764489/), and a German study found that during the first 15 months of the pandemic, there were no deaths from Covid-19 amongst healthy children in the 5-11 age group (https://www.medrxiv.org/content/10.1101/2021.11.30.21267048v1.full.pdf). Covid-19 poses a similar risk to children as the seasonal flu [2] and statistically speaking, your child is more likely to be hit by lightning than to die of Covid. [3]

3. What's the difference between the Covid vaccine and other childhood vaccines?
Many parents who have happily vaccinated their children in the past are questioning (or saying no to) Covid mRNA vaccines like the Pfizer one being administered in New Zealand. They understand that comparing these new vaccines with traditional childhood vaccines is like comparing apples with oranges.
The Pfizer vaccine isn’t like most other childhood vaccines that have been around for a long time. It uses completely new, experimental gene-based technologies, where the body’s cells are given genomic instructions to reproduce part of the virus, rather than the standard process of presenting a weaker or inactive virus. [1]
The Pfizer vaccine is the first mRNA vaccine to be given approval for emergency use in humans and nothing is known about the long term effects.[2] The mRNA vaccines are only available via “provisional approval” in New Zealand, they have not been granted full approval. Medications under provisional approval are meant to be used only on a restricted basis to treat a limited number of patients (https://www.medsafe.govt.nz/Medicines/policy-statements/ReminderProvisionalConsent.asp). Phase 3 trials have not been completed, which means the vaccines are still experimental. [5] (The estimated study completion date is 2 May 2023.)
Many experts question whether mRNA injections should even be called ‘vaccines’ as technically they are gene therapies and did not meet the definition of traditional vaccines when they were first released. After the introduction of the Covid-19 mRNA vaccines and the discovery that they do not “prevent disease” or “provide immunity”, the CDC altered the definition of “vaccines” and “vaccination” on 1 September 2021.
Before this change in definition, a vaccine was described as a “product that stimulates a person’s immune system to produce immunity to a specific disease” and vaccination as the “act of introducing a vaccine into the body to produce immunity to a specific disease”.
The CDC now defines vaccine as “a preparation that is used to stimulate the body’s immune response against diseases” and vaccination as the “act of introducing a vaccine into the body to produce protection from a specific disease”.[6]
Dr Robert Malone, scientist and co-creator of mRNA technology, has been speaking out about the dangers of the Covid-19 mRNA vaccines and in particular about the damage the spike protein in the vaccine can cause in the body. He has called for a halt to the Covid-19 vaccine rollout.[7]

4. What are the long-term effects of the vaccine?
Nobody knows what the medium to long-term effects from the Pfizer vaccine will be because there is no medium or long-term safety data available. The Pfizer vaccine was authorized for 12–15-year-olds based on just two months of data [1], and Pfizer trials for 5-11 years olds included follow up from just 17 days to 2 months ( https://www.nejm.org/doi/full/10.1056/NEJMoa2116298) Medical trials for vaccines normally take several years. [2]
We don’t know if there will be adverse side-effects that will emerge after one year, five years, 20 years or 50 years because there is no medium to long term safety data available for any of the mRNA vaccines in use.
We do know however, that any long-term effects from these vaccines are far more consequential for children and young people, who have a remaining life expectancy of 55 to 80 years, than for adults, particularly the elderly. [3]
Concerns have been raised about autoimmune disease, which can take years to manifest, and possible effects on fertility and the placenta and the reproductive organs of both boys and girls. Long term effects may (potentially) not be known until they try to conceive. None of the mRNA vaccines have a built-in off-switch to control where they travel in the body and how long they persist there. Published animal safety studies showed traces of Covid-19 spike protein in the brain, heart, and other vital organs, while the European Medicines Agency’s assessment report acknowledged that low levels of mRNA were detected in most tissues.[4]
A paper published in 2021 raised the possibility that mRNA Covid-19 vaccines could trigger prion-based, neurodegenerative disease. [5]
Unsurprisingly, given how quickly it was developed, there is still a lot we don’t know about the safety, efficacy, and quality of the Pfizer vaccine, which was approved by the New Zealand government for use on a small group of people via an ‘authorisation under interim order’.
Bottom line: no health professional in good conscience can look a parent in the eye and say this vaccine is unequivocally safe for their child. They need to wait for the
completion of long-term safety studies before they can say with any confidence that the vaccine won’t cause irreparable harm in the short or long term.

5. Have other vaccines been introduced for emergency use and were they safe?
Yes, there have been other vaccines introduced for emergency use, and no, they weren’t always safe.
History has taught us that pandemic or not, we must always be cautious when rolling out a new medical treatment, to avoid unintended harm.
The swine flu vaccine, Pandemrix, was rolled out in response to the 2009 pandemic. It was later withdrawn after causing over 1,000 cases of narcolepsy in children and teenagers. Public Health England undertook a major study of 4 to 18-year-olds and found that around one in every 55,000 jabs led to narcolepsy. [1] [2]
Dengvaxia, a vaccine against Dengue, was withdrawn in 2017 after 19 children died of possible Antibody-Dependent Enhancement (ADE). [3] These vaccinated children became fatally ill after encountering the real virus.
All previous attempts to develop coronavirus vaccines resulted in Antibody-Dependent Enhancement in the test subjects, so these vaccines were abandoned. ADE has not been ruled out in Covid-19 vaccines, as animal trials have been limited or skipped and there is not enough long-term data on the human participants. [4]

6. Should my child get vaccinated to keep the elderly and vulnerable safe?
Despite their admission that the Pfizer vaccine doesn’t stop a person catching or transmitting Covid, the New Zealand government has used the argument that children should get vaccinated to protect adults, particularly the elderly and vulnerable. This is a new and unethical practice that is not supported by evidence-based research. [1]
Whatever your moral stance is about putting children at risk to protect others, there is no science to back up this rationale of protection.
For a start, children both catch and transmit the virus less than adults. [2][3]
Transmission of SARS-COV 2 from children to adults is minimal and adults who interact with children do not have higher Covid-19 mortality.
In fact, living with children has been shown to reduce the risk for the rest of the household. Studies have shown those over 65 living with children, are less likely to be hospitalised from Covid than those who are not. [4]
We also know that schools are not drivers of transmission. [5][6][7][8] Teachers are at no higher risk from Covid than the rest of the population, despite their daily close contact with large numbers of children.[9]

7. If something goes wrong, will my child get help? Will Pfizer or the government accept responsibility?
No. Pfizer, the manufacturers of the mRNA vaccine being used in New Zealand, are exempt from liability for adverse events related to vaccination. [1]
Which leads to the question: what motivation do they have to make the vaccine safe for adults or children?
If your child is injured by the vaccine, you will not be able to sue Pfizer and they will not have to give you any compensation.
In July 2020, a senior executive of another vaccine company, AstraZeneca, explained why pharmaceutical companies have requested zero liability. “This is a unique situation where we as a company simply cannot take the risk if in…four years the vaccine is showing side effects.” [2]

8. Are there safe and effective treatments for Covid?
Yes. It has become increasingly clear since early 2020 that there are safe and effective prevention and treatment options available, including for children and young people with co-morbidities.
Many doctors have used Ivermectin with great success, both when treating patients and prophylactically (preventatively). [1] Other effective treatments include Hydroxychloroquine, [2] vitamin D [3], vitamin C, [4][5] as well as a number of other repurposed drugs. [6] [7] [8]
The Front Line COVID-19 Critical Care Alliance (FLCCC) have published the i-MASK protocol for prevention and early treatment of Covid-19 (https://covid19criticalcare.com/covid-19-protocols/i-mask-plus-protocol/), and the World Council for Health have also published treatment guidelines for managing Covid at home. [10] Dr Shankara Chetty, a Doctor from South Africa, has treated over 7,000 Covid patients in his outpatient clinic and not one has died from Covid-19. He developed the “8th Day” protocol which can be viewed here: https://8days.org/the-protocol.
Unfortunately, many promising treatments have been dismissed and ignored. Just the discussion of their use is censored on many social media platforms, while the vaccine is promoted as the only option to prevent Covid-19.
We also need to remember that our children have incredible, powerful immune systems that we can rely on and nurture to keep them safe.

9. Immunity – is that a good thing?
Yes. Natural immunity is safer and more effective than a vaccine.
“Natural immunity is robust; it’s complete; it’s durable," says Dr. Peter McCullough, a widely published cardiologist and leading voice on a rational pandemic response. [1]
As children are at minimal risk of serious illness from Covid-19, there is a strong case for letting their own innate immune system fight off any infection. [2] [3]
Natural immunity is likely to last longer than a vaccine and cover a broader range of variants. It will also benefit the wider population, contributing to herd immunity against all variants of the virus. [4] [5] [6] [7]

10. If my child gets vaccinated now, will that be it – job done?
Will our children need three-monthly or six-monthly Covid boosters for the rest of their lives? How many will that add up to in their lifetime? And what effect will all these jabs have on their health and fertility? We just don’t know.
However, it's unlikely they will only need two injections. The New Zealand government has introduced a third injection (“booster”) for adults already and in other countries they are on to shot number four.

11. Will getting vaccinated prevent my child from infecting others?
No, the Pfizer vaccine does not prevent a person from catching or passing on the SARS-CoV-2 virus.
The USA’s Centers for Disease Control and Prevention (and our very own Ministry of Health) says a fully vaccinated person can still get infected and spread the virus to others.
A study published in The Lanced (29 October 2021), compared viral transmission to household contacts from vaccinated and unvaccinated individuals. The authors found no difference in transmission between these two groups
https://www.thelancet.com/action/showPdf?pii=S1473-3099%2821%2900648-4

12. Does the vaccine work against Omicron?
The current Covid vaccines were developed based on the genetic code of the original “Wuhan” or “Wild type” variant. This was the variant that was first discovered in Wuhan in 2019. The Pfizer vaccine trials were carried out during the “Alpha” variant era. Since the Alpha variant had not changed much from the original Wuhan
variant, the vaccines appeared to reduce symptomatic disease compared to the placebo (estimates of 95% relative risk reduction were made from the initial trials).
The next big variant to arrive on the scene was the Delta variant, in the middle of 2021. It appears that the Delta variant shows some “resistance” to vaccines, with higher rates of “breakthrough” infections occurring in the vaccinated in the Delta era compared to the Alpha era
https://ajp.amjpathol.org/action/showPdf?pii=S0002-9440%2821%2900480-6
Omicron seems to have taken this “vaccine resistance” to the next level. A UK Health Security Agency report states that vaccine protection against mild disease has largely disappeared by 20 weeks after double vaccination. Even the booster doesn’t help much, with 65-70% protection after the booster dropping to 45-50% after 10 weeks. The authors state that “Omicron displays substantial immune evasion properties”.
Israel, a country that has already administered the fourth shot to some of it’s population, is currently experiencing the highest infection rates in the world
Should we be living in fear of Omicron? The mainstream media would have us think so. However, the UK Health Security Agency report that Omicron is less severe, leading to less hospitalisation than Delta. The Royal College of Paediatrics and Child Health (UK) stated that Paediatricians are not reporting Omicron to be a more serious or severe disease in children and young people. Very few children and young people who are admitted to hospital with Omicron need intensive care: